Effective acute pain management in austere environments facilitates patient evaluation, packaging, and transport, processes that are often challenging without adequate pain control. In remote or resource-limited settings, the optimal pain medication should be compact, lightweight, durable, have a convenient temperature storage requirement, be nonsedating, possess a wide therapeutic window, be available in multiple formulations, and present no risk of abuse. While no current medication fulfills all these requirements, suzetrigine (Journavx®), a novel selective sodium channel blocker, may represent progress toward optimal pain management in wilderness medicine.
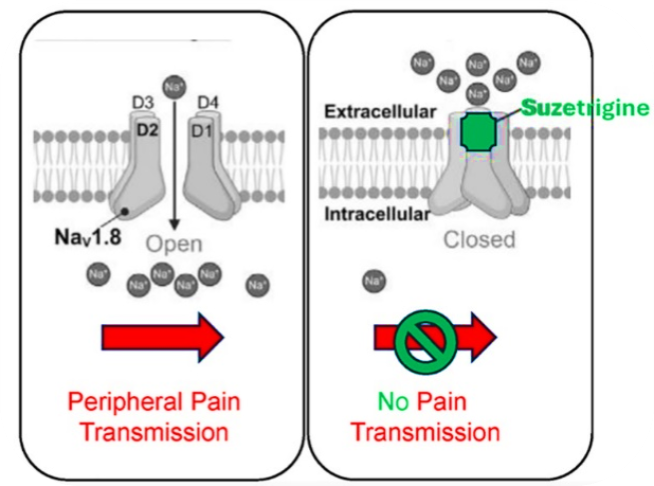
Suzetrigine mechanism of action at receptor level
Suzetrigine (Journavx®), the first non-opioid analgesic approved in a new class in 25 years, is a highly selective oral sodium channel 1.8 blocker (NaV1.8), was approved in January 2025 for the acute management of moderate to severe pain in adults. By stabilizing NaV1.8 channels in peripheral nociceptors, suzetrigine selectively suppresses pain signals while avoiding opioid-like effects due to limited CNS penetration .
Suzetrigine was approved based on the results of two randomized controlled clinical studies in the treatment of moderate to severe acute pain after full abdominoplasty and bunionectomy. More analogous to a wilderness trauma setting, a phase 3 open-label safety study in 256 patients with moderate to severe acute pain, including surgical and nonsurgical causes, found suzetrigine generally safe and well tolerated, with no serious adverse events. While clinical effectiveness wasn’t rigorously assessed, 83.2% rated the drug as good, very good, or excellent for treating pain.
For acute moderate to severe pain, the loading dose of suzetrigine is 100 mg on an empty stomach (one hour before or two hours after food). Maintenance doses of 50 mg are given every 12 hours starting 12 hours after the loading dose, with or without food. Tablets should be swallowed whole. The onset of action is about 2 hours, which is slower than some oral pain medications and much slower than parenterally administered drugs (IV/IM), making it less usable for unstable patients and those with rapidly evolving pain. Suzetrigine should be stored at room temperature, 68°F to 77°F (20°C to 25°C) with excursions permitted to 59°F to 86°F (15°C to 30°C), convenient except for travel in extremes of temperature.

Suzetrigine mechanism of action in body
Suzetrigine is metabolized in the liver by CYP3A and excreted in feces and urine. It is contraindicated in patients receiving strong CYP3A inhibitors (e.g., ritonavir, ketoconazole, and grapefruit juice) due to the risk of suzetrigine toxicity. Strong CYP3A4 inducers (e.g., rifampin) may lead to decreased effectiveness of the drug. Individuals with hepatic impairment should have their dose adjusted or avoid use of the drug altogether. Suzetrigine interacts with hormonal contraceptives; therefore, non-hormonal or alternative contraceptive methods should be used during therapy and for 28 days after the last dose of the drug. Additionally, local anesthetics, such as bupivacaine or ropivacaine, act as non-selective sodium channel blockers - although studies are limited, when used with suzetrigine, they demonstrate additive inhibition of NaV1.8, which may enhance peripheral nerve blockade while minimizing central nervous system or cardiovascular toxicity.

Suzetrigine oral tablet
Although clinical studies of suzetrigine included individuals aged 65 years or older, insufficient data prevent determining whether these patients respond differently to suzetrigine, however, pharmacokinetic analyses indicate that age does not necessitate changes in dosing. There are no data in pediatrics, those with severe renal impairment (eGFR <15 mL/min), as well as pregnant and lactating adults, creating a significant gap for wilderness responders who may treat patients of any age.
Clinical trial data, including double-blind, placebo-controlled, and active-controlled studies, demonstrate that suzetrigine has a favorable safety profile. The most frequently reported adverse effects were: muscle spasm, skin rashes (1%), reduced eGFR (3%), and elevated creatine phosphokinase [CPK] (1-3%); in wilderness settings, the risk of elevated CPK should be assessed in patients receiving suzetrigine as some individuals may be predisposed to rhabdomyolysis due to nutritional status following extreme physical exertion.
The 2024 Wilderness Medical Society Clinical Practice Guidelines emphasize that clinicians should manage acute pain to achieve adequate relief, support the treatment team, and account for the constraints of austere environments. Pain management remains challenging due to limited monitoring, restricted access to patients, reduced capacity to manage adverse effects, and difficulty reassessing patients during transport. The opioid problem in remote medicine is not primarily about addiction: opioids cause respiratory depression, nausea/vomiting, sedation, and impaired cognition, all of which compound rapidly in patients who are cold, injured, and hours from definitive care. The ability to provide effective moderate-to-severe pain relief without those effects is what wilderness and tactical medicine has lacked. Suzetrigine has no adverse CNS, cardiovascular, or behavioral effects, and no evidence of addictive potential or dependence, distinct positives in a wilderness setting.
While suzetrigine is a promising addition to choice of pain medications for multimodal pain management in wilderness settings, more evidence is needed to confirm its effectiveness in pain, period, and in this case, for specific injury types encountered in these settings: this includes extremity fractures, musculoskeletal injuries, cold injuries, bites, burns, and visceral pain. Administration is restricted to patients who are alert and able to swallow, which may not always be feasible in austere situations.
The cost of suzetrigine is a major consideration at this point – it is expensive compared to generic opioids and NSAIDs, and prehospital/wilderness kits operate on tight formulary budgets. A cost-effectiveness analysis failed to demonstrate a net health benefit of suzetrigine compared to oral NSAIDs when both were combined with nonsystemic therapies (heat therapy or local anesthetic). The cash cost for thirty 50mg tablets is close to $500, and while savings cards are offered by the manufacturer, this would only be beneficial for an individual patient – not if this were to be purchased for a group medical kit.
In summary, suzetrigine has not been recommended in any wilderness medicine guidance yet. It could be useful in wilderness settings for:
- Acute musculoskeletal injuries such as sprains, fractures, soft tissue injuries
- Post-traumatic pain after splinting or packaging and during long evacuations
- Mild to moderate pain when NSAIDs don’t provide sufficient pain relief but opioids are not desirable (i.e., impaired LOC risk, long carry, single-rescuer scenarios, patient history of opioid use disorder)
- For transport in a medical kit during international wilderness travel, as the procurement and transport of opioids outside the United States is restricted
As wilderness medicine pain recommendations are reviewed and updated over the next several years, suzetrigine will likely appear in discussions as another non-opioid option for moderate-to-severe pain management in austere settings.