NASA’s all male engineer team famously offered 100 tampons to Sally Ride in 1983 on mission STS-7 for one week in space. Innocently asking: “Is that the right number?”
When women plan expeditions, the packing list includes more than dive gear, crampons, and down jackets. It also includes the question: What do I do about my period? Whether it’s a summit push on Aconcagua, a month of fieldwork in the Himalaya, or a dive boat, menstrual management is an expedition logistics issue. It can dramatically affect comfort, hygiene, and safety. Add the physiological stresses of high altitude, dehydration, extreme temperatures, and disrupted sleep, and menstrual management is an important step in operational readiness.

Photo of multiple generations of women on expedition courtesy of: Dr. Linda Keyes taken by Raphaela Pichler
A 2024 review article in High Altitude Medicine & Biology, by Dr. Lenka Harokova, Dr. Linda Keyes (past president of the Wilderness Medical Society), and colleagues supported by the UIAA (Union Internationale des Associations d'Alpinisme) Medical Commission combed through over 7,000 research papers to identify what’s known about hormonal contraception and menstrual cycle control at high altitude. The result: a distilled set of recommendations.
They analyzed 17 relevant studies and found no convincing evidence that hormonal contraception- whether combined estrogen-progestin pills (OCPs), progestin-only methods, or long-acting reversible devices- impairs acclimatization, increases the risk of acute mountain sickness, or diminishes performance at altitude. There’s no data suggesting that the pill, patch, or implant interferes with oxygen adaptation or summit success. It is important to differentiate between OCPs and other forms of menstrual suppression like IUD and long acting injectables as the side effects and risks vary between these options. For example, gastroenteritis poses no issue for those using an IUD or injectable contraception, but I heard multiple anecdotes that even a brief episode can trigger breakthrough bleeding in women on OCPs.
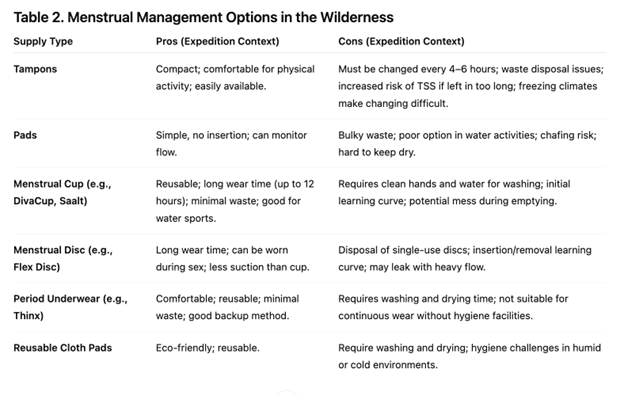
Ray, Foster-Johnson, and Crockett surveyed 620 female backpackers to understand hygiene and menstrual management practices during long-distance expeditions. They found that reusable products were commonly used for both menstruation and post-elimination hygiene, though some were linked to higher reports of UTIs, vaginitis, diarrhea, and skin irritation. Overall, most strategies were safe, and maintaining a consistent hygiene routine was protective. The authors highlight the need for further research on whether female urinary devices contribute to UTI risk and how technique adjustments might reduce symptoms.
What Do the Experts Say?
Dr. Shilpa Gajarawala, PA-C, DMSc, a women’s health specialist at Mayo Clinic in Florida, recommends:
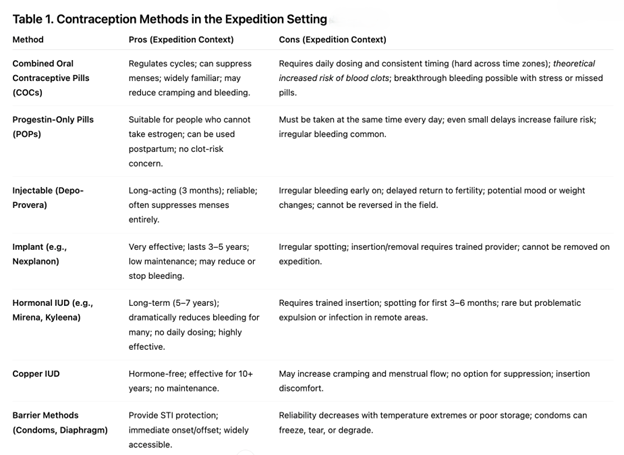
If you’re heading out on a 12-week expedition, it’s totally reasonable to want to suppress your period and it’s safe for most people. A lot of women use continuous birth control pills, the medroxyprogesterone acetate shot or an IUD to skip their cycle. The key is to start early, like a couple of months before the trip, so your body can adjust and you’re not dealing with surprise bleeding in the middle of nowhere. It’s important that there’s no contraindication to therapy. If a woman decides not to suppress, that’s fine too…just plan ahead. Menstrual cups are handy because you don’t have to pack a ton of supplies, but they do take some getting used to. Tampons and pads work too - just make sure you’ve got a system for staying clean and packing out waste. There are no major health risks with suppression short-term, but it’s worth a quick chat with your gyn to find what is safest for you.

Dr. Shilpa Gajarawala with husband Nik. (Shilpa Gajarawala)
Cycle Control as Performance Medicine
The UIAA review emphasizes that the most effective method is the one a woman is already using. Expedition medics are advised not to recommend last-minute switches in hormonal methods solely for travel. For those hoping to suppress menstruation during extended expeditions, longer acting or non-oral methods such as hormonal IUDs, subdermal implants, or depot injections may offer advantages in settings where vomiting, diarrhea, or disrupted schedules complicate oral dosing.
Menstrual irregularities can occur, even with hormonal regulation, due to stress, weight loss, and environmental extremes. Women are encouraged to plan ahead with their medical team. Most of the women I anecdotally surveyed who wanted to suppress their menstruation on expedition were successful.
The Clot Question
Perhaps the most persistent concern involves venous thromboembolism (VTE), especially while taking OCP’s in a hypobaric hypoxic environment (at altitude). Prior concerns that hypoxia itself can theoretically promote hypercoagulability but this has not been proven to be an independent risk factor for VTE. Reassuringly, multiple review studies have found very few documented VTE events among women at altitude and none that conclusively tied contraceptive use to thrombosis. The absolute VTE risk for healthy, non-smoking women remains low.
Dr. Noemi Welsch, an OB-GYN and founder of Women’s Health in the Outdoors, underscores the importance of pre-expedition planning, “Expedition conditions can compromise the reliability of oral contraceptives either to illness, temperature changes, hydration status, or schedule disruption - so long-acting options like IUDs or implants may be preferable to continuous OCP use to suppress menstruation. Ultimately these may be safer and more practical in the field.”

Dr. Noemi Welsch of Women’s Health in the Outdoors. (Noemi Welsch)
Experts agree that conversations about contraception and menstrual suppression belong in early pre-expedition planning. “We normalize gear checks, immunizations, and altitude meds,” Gajarawala adds. “We are normalizing menstrual management with the same professionalism. Women should feel welcome to ask their medical team about this.”
So…What About Marine Expeditions? Sharks?
I get this question a lot from my patients and friends. Although sharks possess a highly sensitive sense of smell and theoretically could detect menstrual fluid in the water, there is no credible scientific evidence showing that women are more likely to be attacked by sharks while menstruating. Marine experts note that menstrual fluid is not simply “blood” but is mixed with uterine lining, mucus, and other secretions, and the small volume released is quickly diluted in large bodies of water making it unlikely to act as a meaningful attractant. Therefore, while standard safety practices (such as avoiding swimming at dawn/dusk, staying clear of areas with fishing/chumming, and not swimming with active bleeding wounds) remain important, menstruation itself does not appear to increase shark-attack risk.

The author on assignment. (Sarah Spelsberg)
So…What About Bears?
There is no scientific evidence that Black bear (Ursus americanus) or Grizzly bear (Ursus arctos horribilis) are more likely to be attracted to menstruating women in wilderness settings. A controlled study found that wild black bears exposed to used tampons and to menstruating women “essentially ignored” the odors, and no attacks on menstruating women were recorded among the sampled data.
Field Lessons and Practical Takeaways
For clinicians advising expeditioners, the take-home points are straightforward:
As summarized in Table 3 of the Horakova et al. (2024) review, best practice for women using hormonal contraception (HC) during travel and high-altitude expeditions is to maintain their current method whenever possible and to start any new regimen at least three months before departure to reduce breakthrough bleeding and thrombotic risk. HC can be safely used for menstrual cycle control during travel, provided dosing times are adjusted consistently across time zones. Clinicians should counsel on proactive measures such as carrying sanitary supplies, managing breakthrough bleeding with NSAIDs, and recognizing the limited antibiotic interactions that truly impact oral contraceptive efficacy (rifampin and rifabutin). For women initiating contraception before high-altitude exposure, nonoral progestogen-only formulations (implants or depot injectables) may offer superior stability and safety due to minimal thrombotic risk and lower bleeding irregularities. Travelers using combined estrogen-progestin methods should receive education on venous thromboembolism (VTE) prevention—staying warm, hydrated, mobile, and avoiding tight clothing or smoking. Finally, as emphasized by Horakova et al., and every other specialist with whom I spoke: both partners share responsibility for pregnancy and STI prevention, reinforcing an approach that integrates physiological safety with shared decision-making and preparedness in expedition environments.
The View Forward
The UIAA review also highlights the lack of sex-specific data in altitude research. Despite more women summiting peaks and leading expeditions than ever before, menstrual health remains an afterthought in historical study design. Future research can examine hormonal metabolism, clotting profiles, and performance variables across different contraceptive methods in hypoxic conditions. For now, the message is clear: hormonal contraception appears to be safe and compatible with high-altitude adventures and other extremes. Menstruation can be suppressed and managed thoughtfully. Expedition medics should provide individualized counseling, encourage early planning, and debunk myths that keep reproductive health off the mountain. Women’s physiology isn’t a barrier to performance! As more of us push into the planet’s extremes, so will our understanding of hormonal health in those environments.