Hearing the word “pressure” may immediately bring to mind the infamous bass line from the legendary Queen/Bowie song. Or even the synthesizer-laden rock anthem by Billy Joel. But today, we are talking less about famous songs and more about pressurized chambers used for treatment in various wilderness medicine scenarios, including altitude and dive medicine. In this article, we will review the differences between chambers and the indications and protocols for treatment in each setting.
Altitude Sickness and the Gamow Bag
The Gamow Bag (brand name) is a portable, soft-sided pressure chamber that can be used in the setting of mountain medicine for the emergent treatment of altitude-related illnesses, such as acute mountain sickness (AMS), high altitude cerebral edema (HACE), and high altitude pulmonary edema (HAPE). In terms of pressure chambers, it is one of the simplest forms. Made of lightweight, durable nylon material with a urethane coating, this is the most portable pressure device available. Most bags hold a maximum pressure of two pounds per square inch (2 PSI), which is enough to simulate anywhere from 3,000 to 9,000 feet (1,000 to 3,000 meters) of descent in an altitude setting.

Gamow bags are portable, able to be carried in a backpack.
This version of a hyperbaric chamber is meant only as a temporizing measure, particularly when rapid descent at altitude is hampered by extreme weather or severity of symptoms. A portable pressure chamber of this kind is not intended to be used with supplemental oxygen; the pressure alone should suffice as treatment for the patient to provide a higher partial pressure of oxygen. Once a patient is lying inside, the chamber is closed with the zipper. The chamber can be secured to the ground with the straps in the event of weather concerns. The foot pump is attached to the intake valve and is pumped up to 2 PSI, which creates a differential with the ambient pressure. As a patient exhales carbon dioxide, a relief valve releases air to maintain pressure at 2 PSI and fresh air is pumped in with the foot pump at 10 to 20 pumps per minute, necessitating constant attendance. Though a useful tool, these bags limit patient access, making frequent assessments of mental status necessary, and pose a risk of developing severe re-entry symptoms if material failure occurs or emergent access to a patient is required.
Though some may consider these bags for use in the treatment of decompression sickness (DCS), they are not intended for this use as they are not capable of holding an internal pressure necessary to meet the standard of treatment, usually 2 atmospheres (ATM), approximately 29 PSI, or higher. While these have been shown to work well in the treatment of altitude illnesses and are generally stocked as emergency equipment in mountain clinics and ski resorts, their use beyond that setting is limited.
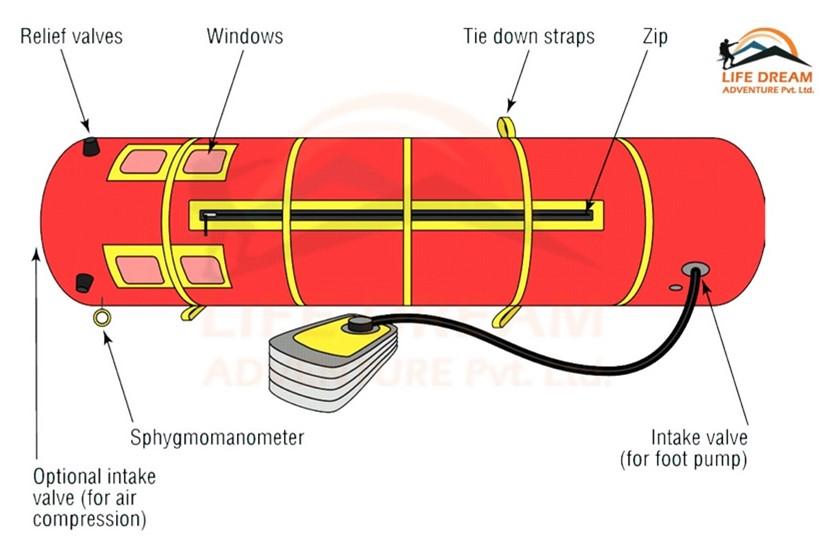
Parts of a Gamow bag. The bag consists of a chamber in which the patient lies, a zipper, small observation windows, tie down straps, an intake valve with a foot pump, a pressure manometer, and a relief valve.
Hyperbaric Oxygen Therapy (HBOT)
Underwater exploration, diving physiology, hyperbaric physics, and dive medicine have a fascinating history. Humans have been undertaking underwater excursions for centuries, and over time have learned much about the human body under pressure. (For a more detailed historical review, check out the four part series “Under Pressure” in the WMM core column The Waterline).
What we know today about treatment of DCS and other dive-related illnesses and injuries stems from an observation in the 1800s of construction workers laboring inside pressurized, underwater chambers, called caissons. As the stories go, construction workers who spent significant time in these environments for work and then returned to the surface were experiencing symptoms such as muscle pains (“the bends”), shortness of breath, and chest pain (“the chokes”). It was observed at the time that returning these workers to the pressurized environment would quickly relieve symptoms. Once the exact cause of their symptoms was worked out by physiologist Paul Bert in 1878, this laid the foundation for the development of modern day hyperbaric oxygen chambers and the treatment protocols used in current management of DCS.
The early 1900s saw significant interest in hyperbaric physiology and the development of hyperbaric chambers, with successful treatment of construction workers and divers being conducted by the 1930s, including use by the US Navy. This led to a period of military research that accelerated refinements in hyperbarics and established treatment protocols that are still used today, namely the USN TT5 and TT6 tables.
Early chambers were large, bulky, made of heavy steel, and offered limited access to chamber occupants receiving treatment. Several early chambers also used only ambient air instead of oxygen, which altered outcomes in treatment. Today, HBOT involves protocols in which patients are “descended” to an equivalent seawater depth of 2-3 ATMs of pressure while breathing 100% oxygen. Protocols include prescribed oxygen breaks to reduce the risk of oxygen toxicity and slow ascents with frequent neurologic and symptom evaluations to determine efficacy of treatment. Hyperbaric chambers are used primarily in hospital settings, dive research, and for military and space applications.
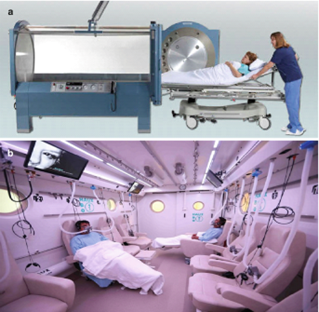
HBOT chambers can either be monoplace, for single occupancy use, or multiplace, allowing for treatment of multiple patients at once.
Hospital-based HBOT chambers are generally large, stationary structures constructed of permanent materials. They can be single or multi-occupancy capacity, and they have multiple treatment indications, including carbon monoxide poisoning, burns, chronic or necrotizing wounds, compartment syndrome, air or gas emboli, osteomyelitis, and intracranial abscesses, in addition to DCS. Emerging evidence also shows some efficacy in HBOT treatment of frostbite injuries. In contrast to a low pressure system such as the Gamow bag, hospital chambers have the capacity to pressurize up to 6 ATM, though a majority of treatments only reach about 2.8 ATM with the TT5 and TT6 tables “diving” to 60 feet of seawater.
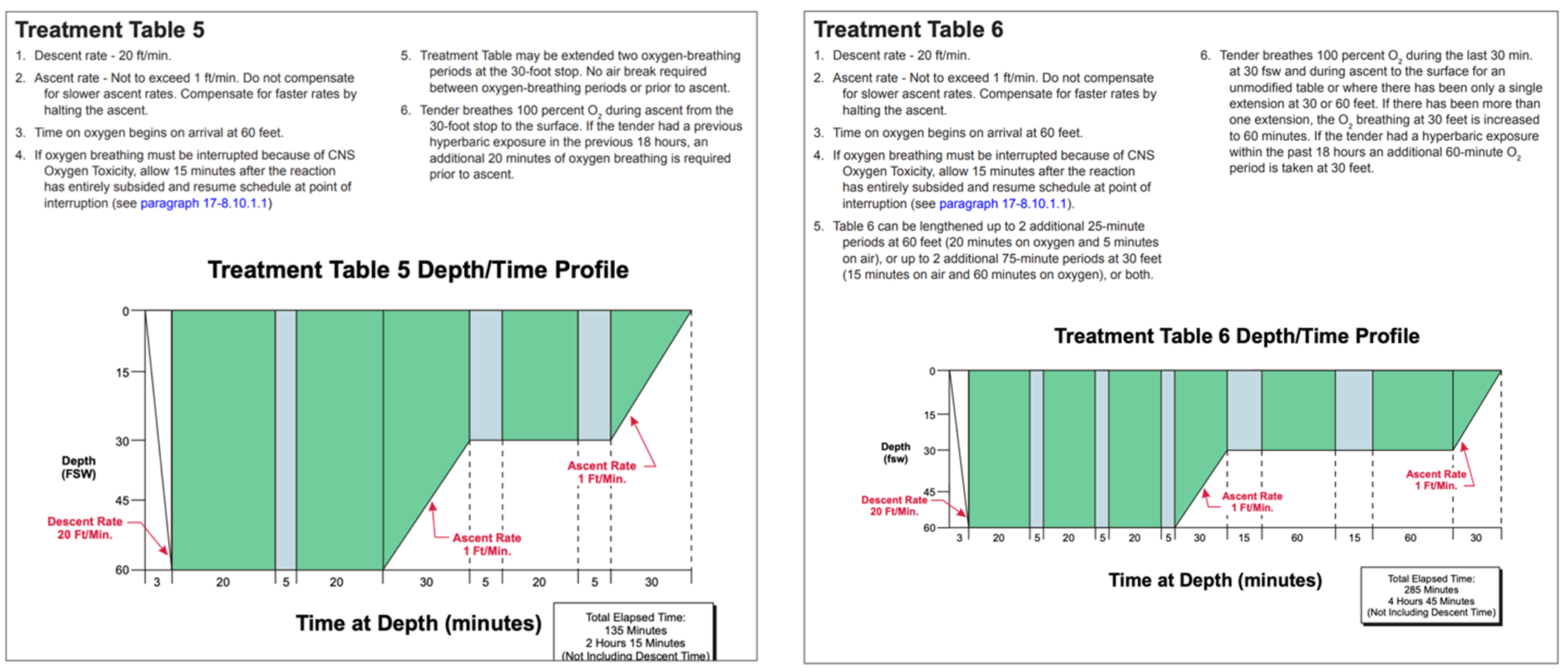
The USN TT5 and TT6 tables are the treatment protocols used in the majority of DCS cases. Based on the charts above, patients are taken to 60 feet of seawater over the course of 3 mins, given 100% for 20 mins, followed by a 5 minute oxygen break, and the treatment proceeds with administration of oxygen, followed by breaks (blue bars), and slow ascent. Patients are evaluated for resolution, progression, or worsening of symptoms throughout the “dive,” which dictates if additional time is needed at various depths.
These chambers also meet rigorous safety standards established by the American Society of Mechanical Engineers, and fall under the National Fire Protection Association’s Healthcare Facilities Code (NFPA 99) to ensure that risk of fire and explosion are minimized. During treatments, chambers are under the operation of trained hyperbaric physicians and technicians who oversee the implementation of DCS treatment protocols over the course of hours, sometimes days, as determined by the severity of symptoms.
While divers and wilderness medicine providers may rely on the availability of a nearby HBOT chamber for treatment of DCS, there is ongoing concern about the fact that many facilities are no longer offering emergent treatment for dive-related injuries, citing personnel limitations and financial cost. Though the Diver’s Alert Network (DAN) estimates that approximately 1500 HBOT chambers are in operation in the US, only about 67 currently treat dive-related emergencies.
One proposed solution to this problem is the increased development and production of portable HBOT chambers, or hyperbaric stretchers. Though they were developed over 30 years ago, they are still only used primarily by military divers. The Hyperlite 1 is the first stretcher that was produced and is constructed of lightweight materials that can be assembled on-site. It can reach pressures up to 3.3 ATM and offers the capability of providing hyperbaric treatment during flight evacuation. With a limited amount of hospital facilities offering treatment, portable stretchers could offer an alternative solution with treatment available within minutes of recognition of DCS symptoms.

Portable hyperbaric stretcher, Hyperlite I
Other Soft-Sided Chambers
Over the last several decades, hyperbaric oxygen therapy has been marketed in the wellness industry for treatment of TBI, PTSD, and sports recovery. Soft-sided chambers can be accessed at wellness boutiques or purchased for home use. Multiple agencies, including the Food and Drug Administration, Undersea and Hyperbaric Medical Society, and National Board of Boiler and Pressure Vessel Inspectors warn against the use of these chambers, which lack regulatory oversight and have not been proven to be effective as they generally operate at less than 1.5 ATM. There are multiple safety concerns with these devices, making them likely more harmful than good. The Gamow is the only soft-sided chamber that is FDA approved, and only for the treatment of altitude illnesses. If in need of HBOT treatment, it is best to seek medical care from those trained in hyperbaric medicine.

One example of a purchasable, in-home soft-sided hyperbaric chamber.