The sport of rock climbing requires exquisite strength and fine motor movements. The most common injuries seen in rock climbing are tendinopathies (tendonitis, tendon strain, or tendon rupture), muscle strains, and joint sprains, accounting for almost 75% of all injuries. Other injuries include fractures, joint dislocations, lacerations, nerve injuries, concussions, and blunt trauma. Patients are often evaluated by primary care physicians, emergency room physicians, as well as subspecialty providers in sports medicine, orthopedics, and physical medicine and rehabilitation.
Conversely, when rock climbing athletes present to the emergency room with an acute injury, fractures are the most common diagnosis, followed by sprains and strains. Injuries evaluated in the emergency department (ED) setting were more commonly observed in the lower extremities, often seen in the ankle, with the most common mechanism of injury being a fall. Overall, factors associated with delayed recovery from climbing injury include older age and active smoking status, while sex and health insurance status do not show significant differences in recovery times. Prior injury has been defined as a risk factor for injury in rock climbing. Other risk factors for climbing injuries are not well defined, but may include lead climbing, increased age, increased years of climbing experience, higher skill level, and higher climbing intensity.
Overall, 60-70% of injuries in rock climbing occur in the upper extremities, with the majority involving the fingers, hand, and wrist. Sport-specific injuries most often occur in the distal upper extremity due to the significant biomechanical load and positioning required to perform various climbing movements. Fingers are among the most commonly injured structures with the flexor pulley system being the most common finger injury seen in rock climbers.
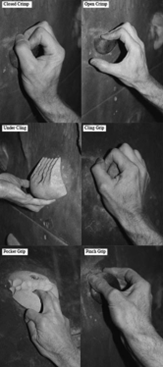
Types of Climbing Grips. Source: Current Sports Medicine Reports
In the forearm, the flexor digitorum profundus muscle (FDP) lies deep to the flexor digitorum superficialis (FDS). Proximally, these muscles attach to the medial epicondyle. Distally, the FDP attaches to the distal phalanx of the second through fifth fingers, while the FDS tendon attaches to the middle phalanx of the same fingers. These muscles allow for flexion of the distal interphalangeal joint (DIP) and proximal interphalangeal joint (PIP), respectively. The flexor pulley system involves multiple bands of fibrous tissue wrapping around the tendons of the FDP and FDS to maintain proper positioning and stability by securing the tendon adjacent to the phalanx. This system allows for a smooth translation of force from the FDP and FDS to the fingers resulting in fine motor movements and finger flexion.
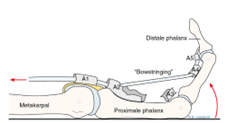
Flexion Mechanism of Finger. Source: SportNetDoc
In total, there are 5 annular (A1-A5) and 3 cruciate (C1-C3) pulleys on each digit. The A2 and A4 pulleys are often considered the most important given their large size and role in preventing bowstringing, a condition where the flexor tendon deviates from its anatomical position resulting in impaired flexion mechanics. The A2, A3, and A4 pulleys have the highest risk for injury, with isolated A2 injury being the most common.
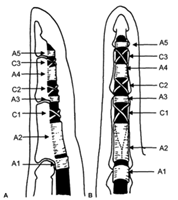
Pulleys of the Finger. Source: Journal of Hand Surgery
Pulley rupture may be partial or complete and may involve a single pulley or multiple pulleys. Bowstringing is typically seen when multiple pulley injuries occur. Patients will endorse feeling or hearing a pop, followed by pain, swelling, and bruising of the finger. Grip strength is often preserved. Eccentric loading of the flexor tendons predisposes climbers to pulley rupture. This is most commonly seen when using the “crimp” grip, where the PIPs are flexed and the DIPs are extended, as this position places high stress on the pulley system.
Diagnosis is made through history and physical examination, with subsequent imaging to assess surrounding structures. Radiographs may be obtained to rule out bony injury, such as an avulsion fracture. MRI can evaluate for various injuries including flexor pulley rupture, tendonopathy, stress fracture, or muscle or ligamentous injury. MRI and US are both effective imaging modalities for diagnosing flexor pulley rupture, with some studies suggesting US be the initial modality of choice due to lower cost, diagnostic accuracy, and ease of access. The normal distance between the flexor tendon from the phalanx is less than 1.4 mm. Diagnosis of pulley rupture is suggested on imaging by measuring the anterior displacement of the flexor tendon from the phalanx of greater than 2 mm. Bodner et al. describe displacement of the flexor tendon from the phalanx of 3 mm during extension and 5 mm at flexion suggests complete disruption, however optimal positioning for ultrasound evaluation has not yet been well defined.
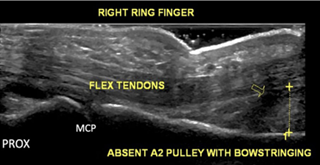
Ultrasound of anterior displacement of flexor tendon. Measured distance = 6.4mm. Source: Diagnostic Imaging of Pulley Injuries
Severity of injury and management is determined using the Schöffl and Schöffl classification system. Grade 1-3 injuries can be managed conservatively, while grade 4 requires operative intervention. A grade 1 injury has no displacement of the flexor tendon and immobilization is not required. Patients with grade 1 injury require therapy for 2-4 weeks and may return to easy sport activity in 4 weeks and full sport activity in 6 weeks. Taping is recommended for a minimum of 3 months. Grade 2-4 injuries require immobilization during the recovery process, ranging from 10-14 days. Grade 3 and 4 injuries require additional protection with a thermoplastic or soft-cast ring. Return to sport for grade 3 and 4 injuries is approximately 8 weeks and 4 months for easy activity, and 3 months and 6 months for full activity, respectively.
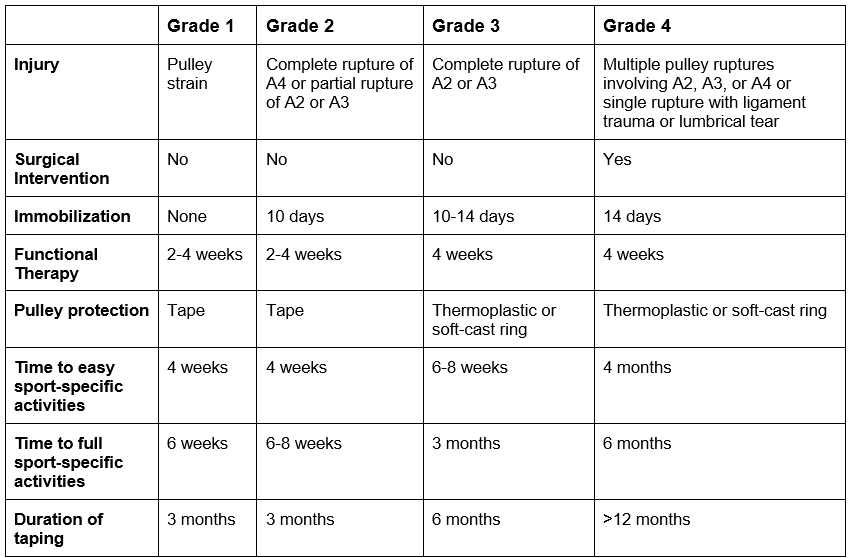
Schoffl Classification of Flexor Pulley Injuries. Source: The Journal of Hand Surgery
Nonoperative management includes rest, ice, anti-inflammatory medications, and external stabilization with bracing, taping, and/or splinting in conjunction with early physical therapy. Corticosteroid injections are generally avoided as they may lead to tendon rupture or delay healing.
When surgery is indicated, reconstruction is favored over repair. Recovery for surgical cases is longer when compared to injuries not requiring surgery. Complications may occur after surgical intervention and include stiffness, synovitis, re-rupture, infection, phalanx fracture, and adhesions. Reoperation occurs in about 6% of patients, often due to development of adhesions. Patients with flexor pulley injuries have favorable outcomes, including regain of normal strength and anatomical alignment, and return to preinjury level of activity. Barring any complications, patients may return to easy sport-specific activities in approximately 4 months. A minimum recovery time of approximately 6 months is required before returning to full sport activity.
The popularity of rock climbing has increased in recent years, especially since its inclusion into the 2020 summer Olympics. Given the exquisite strength and dexterity in conjunction with specific maneuvers required to rock climb, athletes are at risk of unique injuries to the hands and fingers. Finger injuries are among the most common injuries, accounting for 12% of all rock climbing injuries. Flexor pulley injuries are seen more commonly in rock climbers compared to the general public. Injuries of the fingers and hands can result in significant limitations and negative impacts to a person’s functionality and quality of life. Early recognition and focused treatment is of utmost importance.