On August 8, 2024, 28-year-old athlete Lazar Đukić drowned during the CrossFit games in Marine Creek Lake in Fort Worth, Texas. The event shocked the fitness community and left many people asking, “How can this happen to an elite athlete and competent swimmer who was leading the pack?” As of writing (mid-October), the Tarrant County Medical Examiner’s office has not released the cause or manner of death. I am not privy to any details beyond what is available in the public sphere and I do not intend to speculate or opine on Mr. Đukić’s cause of death. Rather, I hope to share some of my experience on how these deaths can occur and how they can be prevented and treated.

Lazar Ðukić, a 28-year-old athlete from Serbia, died August 8, 2024 while swimming across a lake in Fort Worth during the international CrossFit Games.(GoFundMe / Courtesy)
While it is subject to many misnomers, drowning is defined as the “process of experiencing respiratory impairment from submersion or immersion in a liquid”. There are only 3 outcomes to the drowning process, death or survival with or without morbidity, which is typically some degree of brain damage due to lack of oxygen to the brain. Submersion is when the entire head is underwater and immersion is when the airway is obstructed by water, such as someone in heavy surf or whitewater, even if they have an appropriately-sized lifejacket. Analogous to cardiac arrest or stroke, we wouldn’t call someone who survives (with or without morbidity) as having had a “near-stroke” or “near heart attack”. Someone who survives a drowning is said to have had a non-fatal drowning.
One nuance that adds confusion to the understanding and tracking of drowning is identifying the precipitating factors. If someone dies after submerging due a leg cramp, seizure, traumatic injuries, stroke, heart attack, low blood sugar, or any other medical cause, did they drown? Or is their cause of death leg cramp, seizure, trauma, or medical event in a hazardous environment? While this may seem like a purely academic discussion, the critical implication is that effective prevention and treatment strategies address the underlying cause. Something as basic as fatigue, muscle cramp, or a poorly timed breath causing aspiration can trigger drowning in a fit athlete. There is not always a clear answer, but many of the causes of sudden loss of consciousness or sudden cardiac arrest are much more survivable if they occur on dry land, especially if witness by trained medical responders.
The largest case series to date on deaths during USA Triathlon events identified 135 deaths from 1985-2016 with two-thirds occurring during the swim portion. Consistent with the USAT analysis, a 2024 systematic review found cardiovascular disease was the biggest risk factor. Cardiovascular risk factors include clogged coronary arteries (atherosclerosis) or scarring from previous minor blockages that can trigger irregular ventricular dysrhythmias, poor perfusion to the brain, and loss of consciousness. Some of the less common cardiac risk factors that can affect young healthy persons are hypertrophic obstructive cardiomyopathy, pericarditis, or other structural abnormalities, all of which can be seen at autopsy. Lazar’s brother, Luka, posted to his Instagram that the medical examiner categorized Lazar as “extremely fit” and that there were no signs of a “heart attack”. Reading between the lines, this seems to imply that there were no structural abnormalities, areas of dead heart muscle, or coronary occlusions.
Brugada Syndrome, Wolff-Parkinson White, Heart Blocks, Arrhythmogenic Right Ventricular Dysplasia, and long QT syndrome (LQTS) are genetic disorders that can cause loss of consciousness and dysrhythmias in otherwise healthy persons with a structurally normal heart and cannot be detected at autopsy. Long QT syndrome (LQTS) bears additional discussion because swimming is a known trigger. This group of relatively minor genetic mutations can make the electrical system of the heart prone to the polymorphic ventricular tachycardia (Torsades de Pointes). While most of these are inherited and there is often a reported family history of LQTS, 25% of cases are due to a new mutation. Genetic testing is not a routine part of autopsies and even when performed may not provide a conclusive answer. Even if post-mortem genetic testing shows a mutation, that may not have been the proximate cause of death. Conducting a thorough pre-event family history that includes questions about sudden, unexplained death or drowning can identify persons at risk. The American College of Cardiology does not recommend routine, mass 12 lead EKG’s for pre-participation physicals, but there is a role when the family individual history is suspicious for any of the above syndromes.
Another proposed cardiovascular mechanism is “autonomic conflict”. Autonomic conflict occurs when both the sympathetic (“fight or flight” response) and parasympathetic (“rest and digest”) limbs of the nervous system are activated simultaneously, “crossing paths” at the vagus nerve in the heart, and triggering ventricular dysrhythmias. The sympathetic nervous system can be activated by the adrenaline of the race, exertion during exercise, cold water temperatures. The parasympathetic nervous system can be activated by water on the face (“mammalian diving reflex”), water entering the nasopharynx, compression of the chest from tight wetsuits, and breath holding. All these factors are present during swim training, but the sympathetic activation may be more pronounced during a race or competition, triggering ventricular dysrhythmias in otherwise healthy persons.
The next biggest risk factor is the environmental conditions themselves. Open water swims are often scheduled months in advance and the weather on race day may be hotter, colder, choppier, or windier than is safe or anticipated. Event organizers may feel real or perceived pressure to give a green light to events without considering the margins of safety. In training, the athlete may not have encountered these extremes of weather or surf conditions, which increases anxiety and may also complicate rescue efforts. Event organizers should establish acceptable minimum safety standards and utilize local, third-party experts to set safety margins. Participants should be encouraged to set and abide by their own limits.
Safety measures such as participant swim buoys, lifeguards, and safety spotters can enhance competitor safety through prevention, rescue, and treatment. Participants and organizers alike should be aware that not all lifeguards have equivalent training or experience. In addition to certification, lifeguards should be qualified in the specific environment in which they operate. Research is ongoing to address triathlon specific training paradigms. During training, swim with a buddy, use a swim buoy, and communicate your swim plan with the lifeguards.
Rounding out the lower risk causes are respiratory and cerebrovascular diseases. Swimming induced pulmonary edema (SIPE) can be seen in fit swimmers such as triathletes and military special forces recruits. Though the mechanism is not well understood, it is thought to be due to overhydration and breathing on just one side, making one of the lungs “dependent” and more prone to the effects of gravity pulling edema into that lung. While this is often a popular culprit in the lay media, the symptoms are gradual in onset and this rare condition is universally non-fatal if a rescue is performed early. Aspiration occurring during a mass start, pile-up, passing, or a rogue wave can trigger laryngospasm. Fortunately, this is usually transient (think “water going down the wrong pipe at the dinner table”) and resolved by stopping and staying above the water until it passes. Sometimes, this is easier said than done, especially when it was triggered by water conditions as that are not easy to escape and underscore the importance of a swim buoy for self-rescue.
Persons with seizure disorders have an increased risk of drowning. Swimming with a buddy, using a swim buoy, notifying the event safety team, and ensuring antiepileptic drug levels are therapeutic are all critical to creating layers of safety. Questions about personal or family history of seizure disorder and frequency are important components of pre-participant screening. Stroke or other neurovascular causes of syncope are rare and primary prevention is the “treatment” of choice.
It may be some time before Lazar’s cause of death is made public, allowing more targeted prevention and treatment messages. Our hearts go out to his family, especially since their heartbreak is so public. In the meantime, we should understand that there are risks to even elite athletes during swim events (or kayaking, surfing, diving, etc.). Taking appropriate safety precautions during training can reduce risk. During the event, organizers must ensure that there are layers of safety for prevention, rescue, and treatment that match the conditions and scale of the competition.
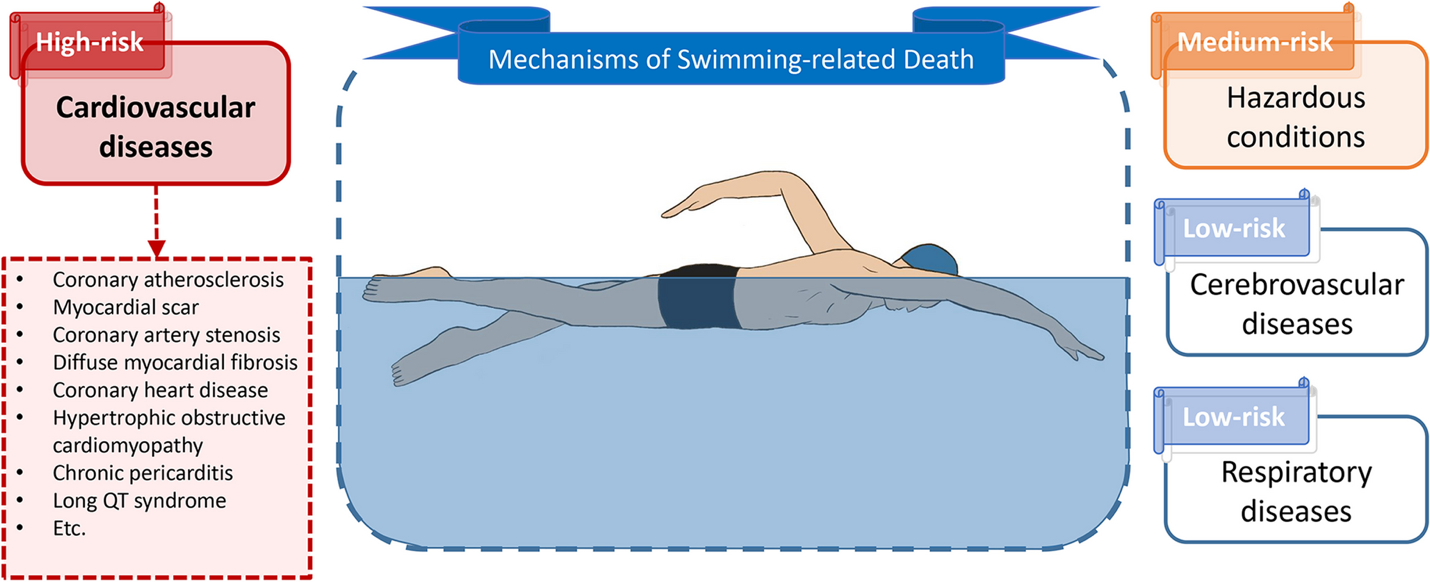
Figure 1: Mechanisms of Swimming-Related Death