The joy of prehospital and wilderness medicine is that no two days are the same. One day you’re providing medical response on a pushbike, the next providing medical support for a free dive/apnea competition. The following is a quick but not an exhaustive tour of some of the fun facts and tips of freediving that are good to know if your office view changes.
Humans have been freediving for thousands of years and it is still a way of life today: from archeological evidence of ancient Greeks freediving both for livelihood and for sport in the ancient Olympics to modern freediving cultures such as Bajan (West Indies) and Haenyeo (South Korea) who have adapted to fish actively and dive repeatedly with breath holds recorded up to five minutes.
Modern-day sport freedivers are pushing physical boundaries, diving to deeper depths and staying under longer, with record breath holds exceeding eleven minutes in static competitions. To push these boundaries, the modern freediver trains to develop adaptive mechanisms.
HYPERVENTILATION
The human body generally functions quite nicely by inhaling the correct amount of oxygen and exhaling the required amount of carbon dioxide. This is regulated by a complex system of central receptors led by the medulla and pons and influenced by peripheral baroreceptors allowing the respiratory system to puff along without mindful input from the human. The main physiologic issue smothering the freediver is that although the diver plans their breath hold, the brainstems’ reflexes still want gas exchange. Cells still crave oxygen and once it is consumed, want to expel the carbon dioxide that is released back into the blood stream. In time, an imbalance of these blood gases causes the apnea diver to have the urge to surface or lose consciousness.
There are several techniques employed by freedivers to ready themselves for this hypoxic/hypercapnic state. All involve risks and education in each technique is paramount to reduce these risks. One side effect of using poor technique is underwater hypoxic blackout or simply “blackout”, previously known as or “shallow water” blackout. This misnomer led to confusion since it can occur at any depth. The definition of blackout is “the loss of consciousness in the underwater swimmer or diver, during an apnea submersion preceded by hyperventilation, where alternative causes of unconsciousness have been excluded”. Several freediving course providers warn against hyperventilation and numerous studies have demonstrated correlation between hyperventilation and blackout in the apnea diver. Effectively, hyperventilation can induce significant hypocapnia and subsequent prolongation of apnea with the risk of developing severe hypoxia. The net effect on the diver is they will feel comfortable without the urge to breath up until the time they blackout. The hyperventilation can be intentional or unintentional. One study of experienced freedivers showed unintentional hyperventilation with increased rate of desaturation during repetitive dives even with a 2.5 min surface interval. The diagram below (Figure 1) demonstrates that the dip in the CO2 curve from hyperventilation allows the diver to reach blackout before they reach the urge to breathe.
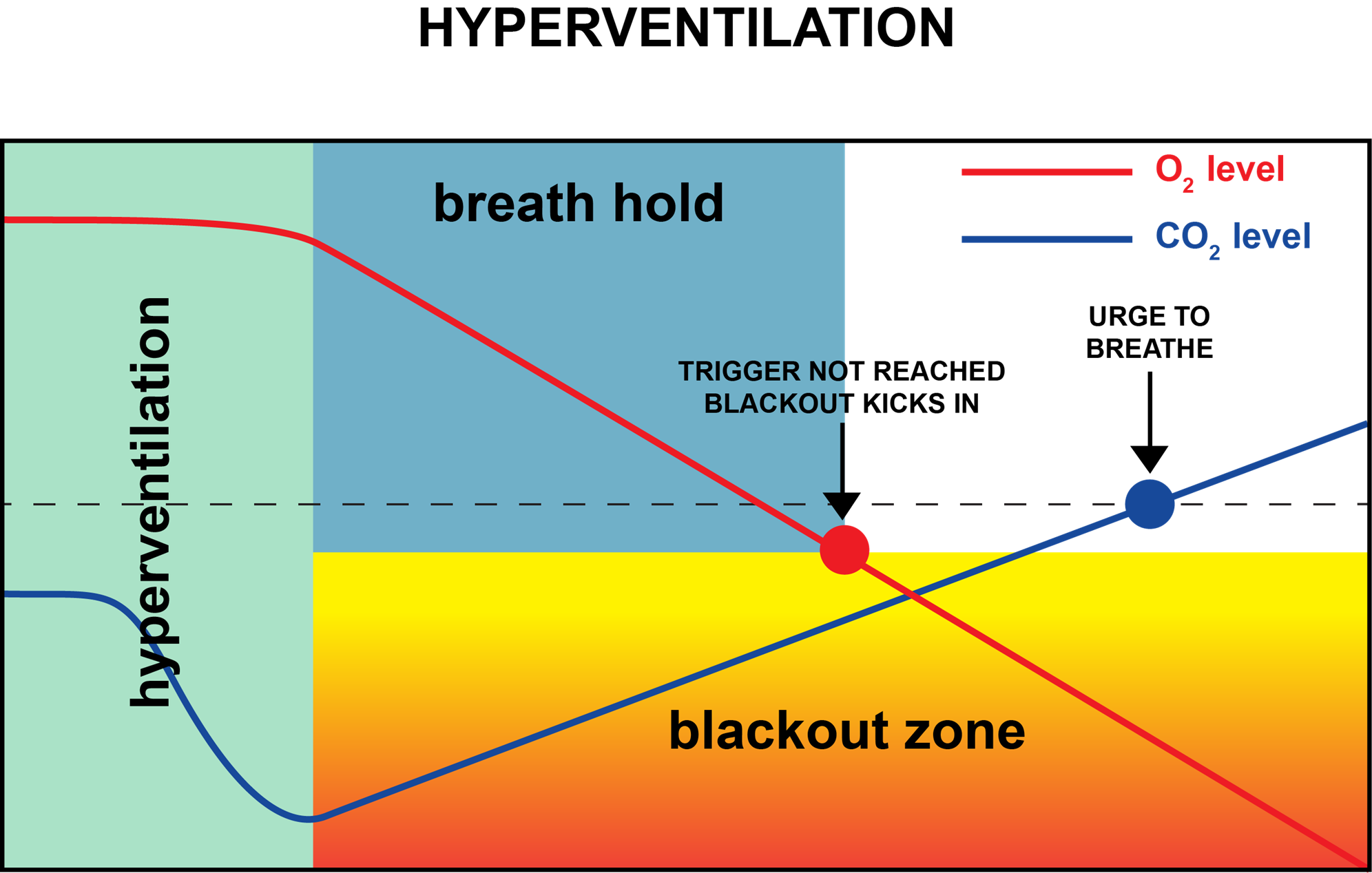
Figure 1: Effect of hyperventilation (source: apneasurvival.com.au Author: Jason Rice)
GLOSSORPHARYNGEAL INSUFFLATION
Another technique utilized by trained freedivers is the glossopharyngeal insufflation or “lung packing”. This technique that looks like weird gulping, uses oropharyngeal musculature to pump air into the lungs. Lung packing has been noted to increase total lung capacity and improve total performance. The downside is hemodynamic changes including increased intrathoracic pressure, reduced cardiac output, and hypotension, which may have detrimental effects if not performed as part of a good technique. These blood gas and hemodynamic changes may get more complex when divers go to depths that exceed the limit of some recreational SCUBA divers. The onsite medic must consider these variations in the pulmonary and cardiovascular systems in divers competing both in shallower depths such as pool competitions and those diving to record depths as diver technique and external hydraulic pressure play a factor at any depth.
PULMONARY BAROTRAUMA
Pulmonary barotrauma is a potential for any freediver, even in the pool setting. Any technique or action that increases intrathoracic pressure, such as excursion at depth or lung packing may expose the diver to potential barotrauma. Increasing depths of elite divers have also been associated with the potential for pulmonary edema or lung squeeze: as the volume of air in the lungs is reduced, there is increased pressure experienced by the pulmonary capillaries, causing increased permeability and fluid in the lungs.
The good news is that freediving, or apnea diving, in the competitive setting is a well-controlled and regulated undertaking that provides education and safety for participants. The Association for International Development of Apnea (AIDA) publishes safety protocols for apnea/freediving competitions and set out minimum clinical standards and equipment required for each type of competition. Several classes or disciplines exist in the competitive free diving world ranging from static competition (literally putting your face underwater in a pool) to the deep dives we see in Netflix documentaries. Training and competition should always be done with a support team in a controlled, professional environment. Breath holding contests in the pool can be more deadly than a professional competition!
As the medical support at an organized event there is very much a reliance on being part of the dive safety team. Well-practiced and coordinated rescue divers both in the competition area but also the warmup areas provide initial contact with distressed diver. The rescue divers must be well-versed in the recognition of a blackout and trained to protect the airway during rescue and to give the initial rescue breaths on the surface. The safety team should have a plan for extrication from the environment. The AIDA provides guidelines for the medical evaluation, extrication, and evacuation pathways to definitive care.
The AIDA also provides a comprehensive list to construct a medical and airway kit. The airway adjuncts in the list have been limited to naso- and oropharyngeal airways. More advanced airways are acceptable if in the scope of the provider, however, as is well documented in the Wilderness Medical Society Practice Guidelines for the Treatment and Prevention of Drowning: 2024 Update, if an unconscious diver is extracted from the water, positive pressure oxygenation is to be prioritized and the most rapid airway adjuncts to facilitate this should be used with consideration of the risks of acquired barotrauma and potentially difficult airways, including beards, body habitus, missing teeth, trauma, and the elderly.

Freediver returned to the surface after 159 meter Dynamic Without Fins event. Note the potentially difficult airway. (Credit Jeff Monro)
The world of the freedive is an interesting physiological and neurological environment that can challenge both our definition of possible and how we see human behavior in extreme environments. In regards to emergent treatments, recommendations contained in the WMS Drowning Guidelines are an excellent resource in conjunction with the AIDA Protocols.

Dynamic Without Fins competitor with safety diver looking on. (Credit – Brisbane Freedivers Club)